Ankle Instability
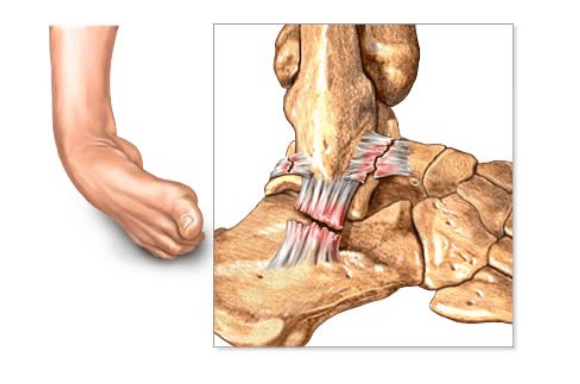
Ankle sprains are one of the most common sporting injuries. Usually the injury recovers with suitable rest and physiotherapy. Ankle instability occurs when the ankle repeatedly gives way during sporting or daily activities. This leads to recurrent ankle sprains, joint pain, swelling, inflammation, and damage to the ligaments around the ankle.
Some people experience ankle pain intermittently, others feel that their ankle aches more often. Recurrent instability episodes can cause damage to the joint surface cartilage, the formation of bony spurs (osteophytes),and arthritis.
Non Operative Management
The first line of treatment for ankle sprains is rest, ice, compression, elevation with painkillers and anti-inflammatories (if tolerated). Physiotherapy is then useful to regain range of movement, strength, balance and joint position sense. An ankle brace may be useful for people who have tried all these measures and experience ongoing problems with sporting or daily activities. Finally, a targeted corticosteroid injection may offer relief from ankle inflammation and help settle symptoms so that physiotherapy can continue.
Operative Management
When all these non-operative measures fail, and recurrent ankle instability becomes an ongoing problem, surgery is indicated. The ankle ligaments are assessed clinically and an MRI scan is often necessary to identify any problems within the ankle joint itself or the tendons and ligaments around the joint.
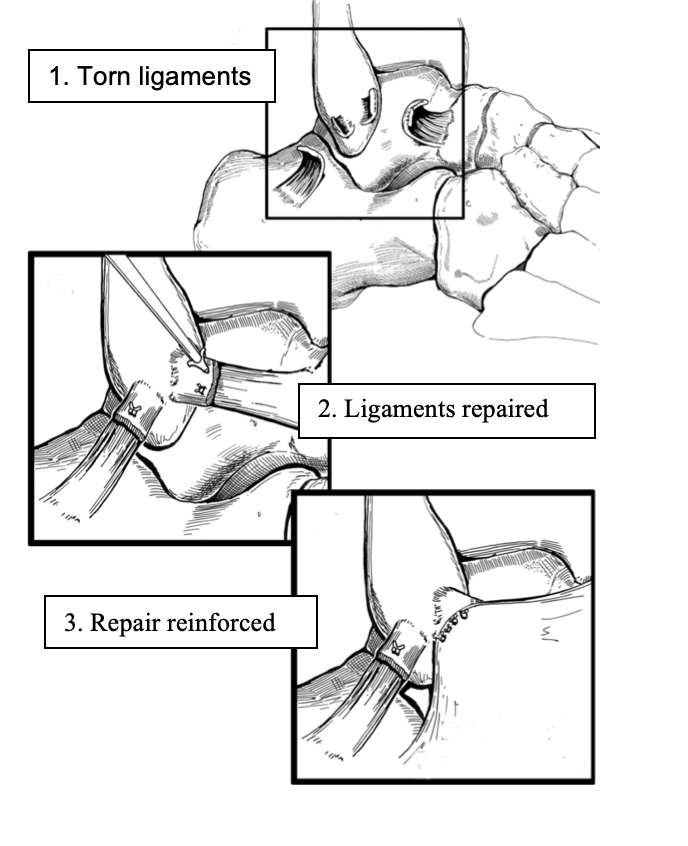
There are 2 components to the surgery. Firstly, an arthroscopy is done through 2 small incisions at the front of the ankle. The joint surfaces are inspected and tidied up if damaged, inflammatory and scar tissue is removed, and any bony spurs (osteophytes) or ossicles are trimmed away. Sometimes a further incision is required to get to the back corner of the ankle if there is a significant problem in that area.
Then an incision is made over the lax or deficient lateral ligament on the outside of the ankle and the ligament is repaired (modified Bröstrom repair), or reconstructed with a tendon graft if necessary, in an anatomical fashion. If indicated, the tendons behind the ankle are inspected and repaired also.
Risks & Complications
No surgery is completely risk free. The risks and complications will be assessed and discussed with you. There is always a small risk of infection, blood clots and anaesthetic problems and measures are taken to reduce these. It is not uncommon to have some minor residual ache from time to time. There is approximately a 5% chance of experiencing problems with recurrent instability and this is usually due to a fresh injury or sprain. Sometimes the ankle heals a bit too well, and then may always be a bit stiffer than the normal side, with a slight reduction in range of motion, but this is rarely a significant problem. A good outcome is achieved in more than 90% of cases.
Recovery Times
Hospital stay Day surgery
Rest & elevation 7-10 days
Crutches 1-7 days
Weight bearing
– As tolerated Day of surgery
– Full By 7 days post-op
Rehabilitation
– 0-4 weeks
– Gentle active ROM
– Calf stretch/strengthening
– Static peroneal strengthening
– 4-8 weeks (with Physiotherapist)
– Proprioceptive exercises
– Theraband
– Further ROM/strengthening
Training/sport from 8 weeks
(with ankle strapping)
Time off work
– Seated 2 weeks
– Standing 4 weeks
Allied resources:
